Build a solid foundation in HIV science (50 questions): This section uses clinical scenarios and feedback-driven questions to help you understand HIV virology, the replication cycle and how the virus progresses from initial to chronic infection. You’ll also review the stages of HIV and how they link to clinical signs, symptoms and decision-making in patient care.
📓 HIV FUNDAMENTALS
HIV is a retroviral disease (RVD) that is usually transmitted vertically (from mother to child) or horizontally (between individuals) via bodily fluids of an infected person in the absence of adequate pre- (PrEP) or post-exposure prophylaxis (PEP); see Table 1 for risk transmission can occur, although rarely, with PreP or PEP. 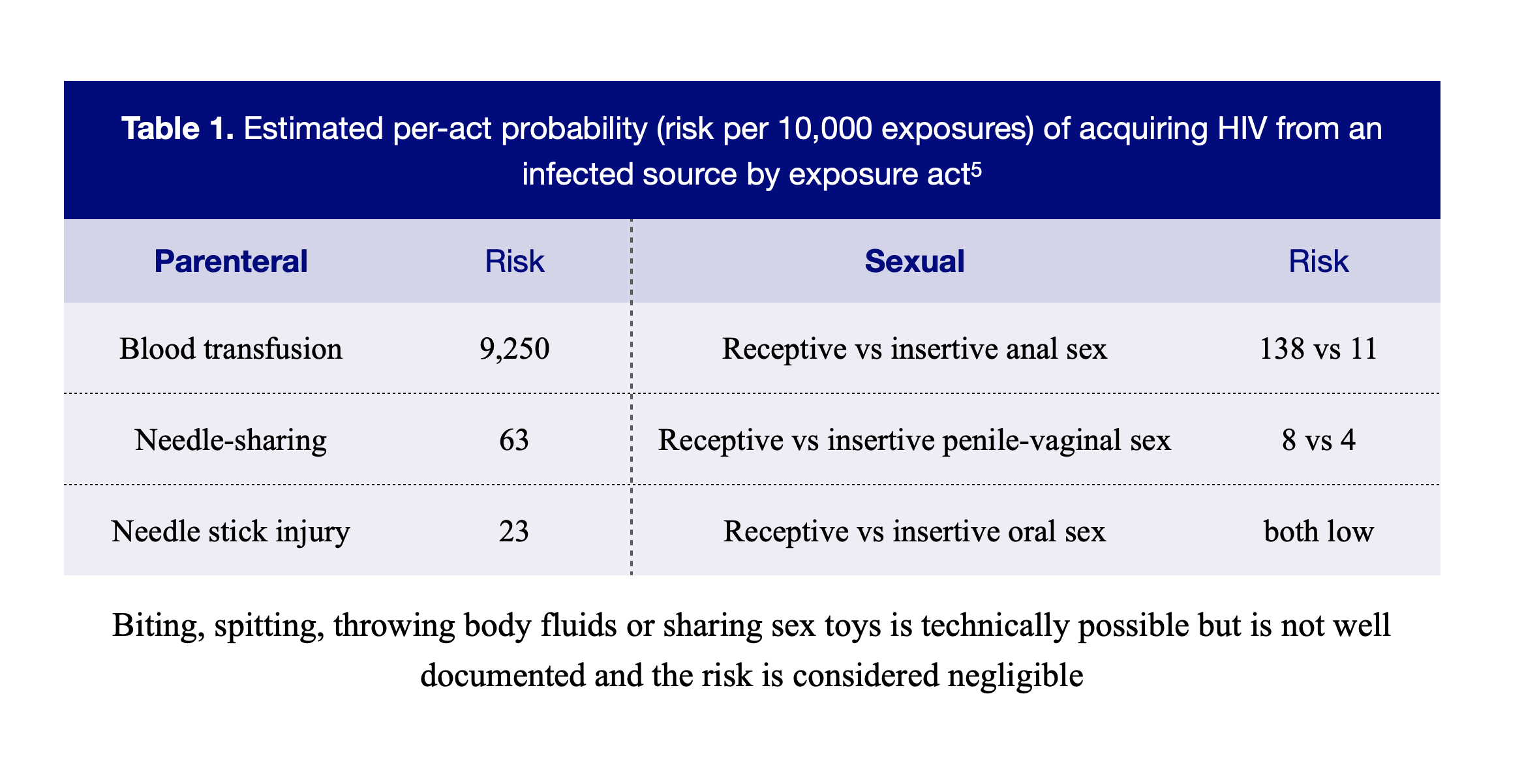 HIV-1 is the most common type, whilst HIV-2 is less common and less infectious. South Africa (RSA) has one of the highest prevalence of HIV in the world. RSA has invested in HIV programs and has made good progress towards the UNAIDS 95-95-95 targets (95% of the population being aware of their status, of which 95% with HIV should be on treatment, of which 95% are virally suppressed).
HIV-1 is the most common type, whilst HIV-2 is less common and less infectious. South Africa (RSA) has one of the highest prevalence of HIV in the world. RSA has invested in HIV programs and has made good progress towards the UNAIDS 95-95-95 targets (95% of the population being aware of their status, of which 95% with HIV should be on treatment, of which 95% are virally suppressed).
Vulnerable groups at risk
- Women, particularly young women and adolescent girls with low socio-economic status (SES), are at risk. Gender-based violence (GBV) is also considered a contributing factor.
- Sex workers: Contributing factors may include the criminalisation of sex work, as this discourages the reporting of rape or assault.
- Men who have sex with men (MSM)
- Intravenous drug users1
- Children and orphans
Risk factors
The aforementioned vulnerable groups, unprotected sexual intercourse, multiple sexual partners, previous or current STI, sharing of IV equipment, mucosal contact with infected bodily fluids, needle stick injuries, and maternal HIV infection.
Pathophysiology:
See Figure 1 and 2 below 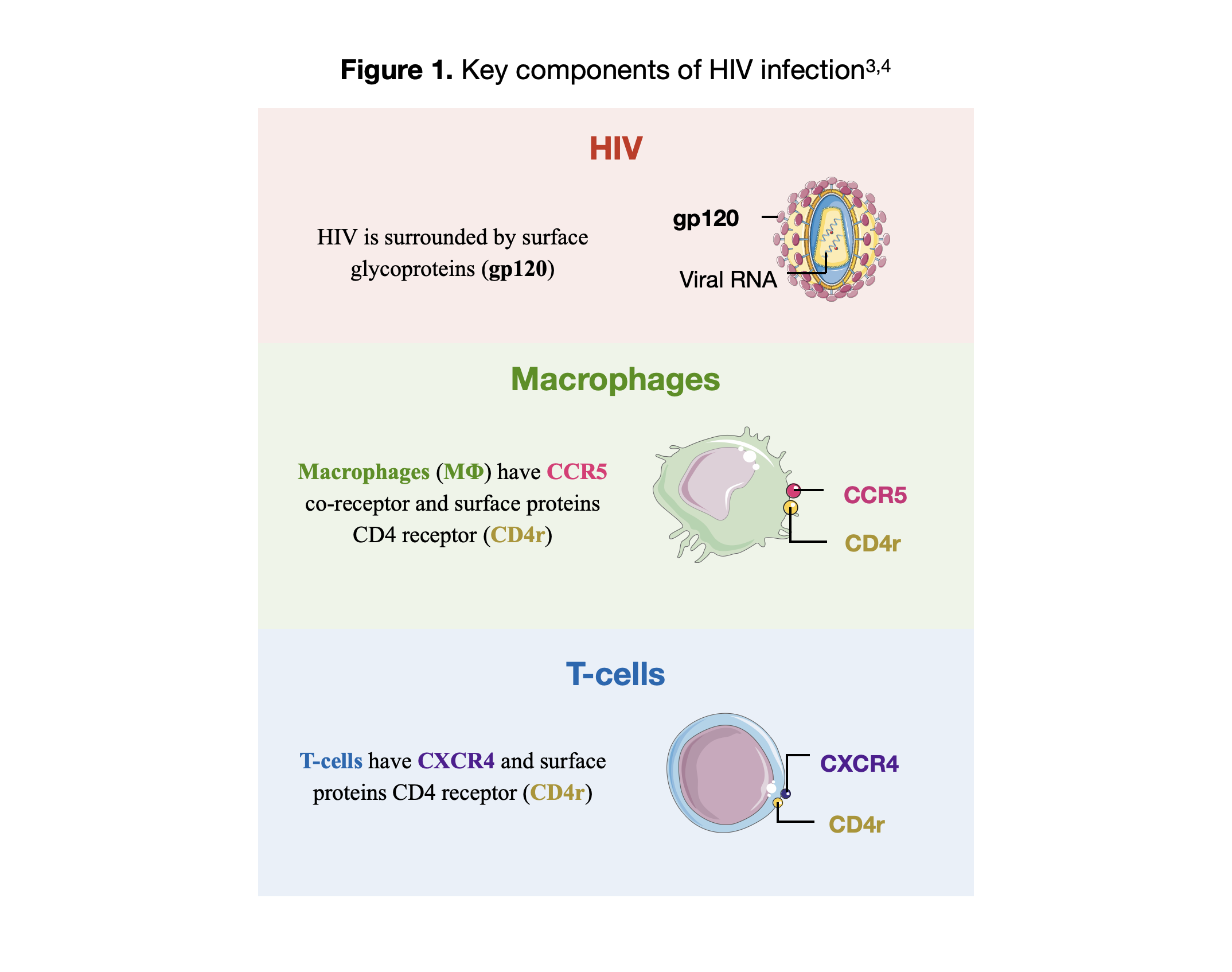 HIV pathophysiology
HIV pathophysiology
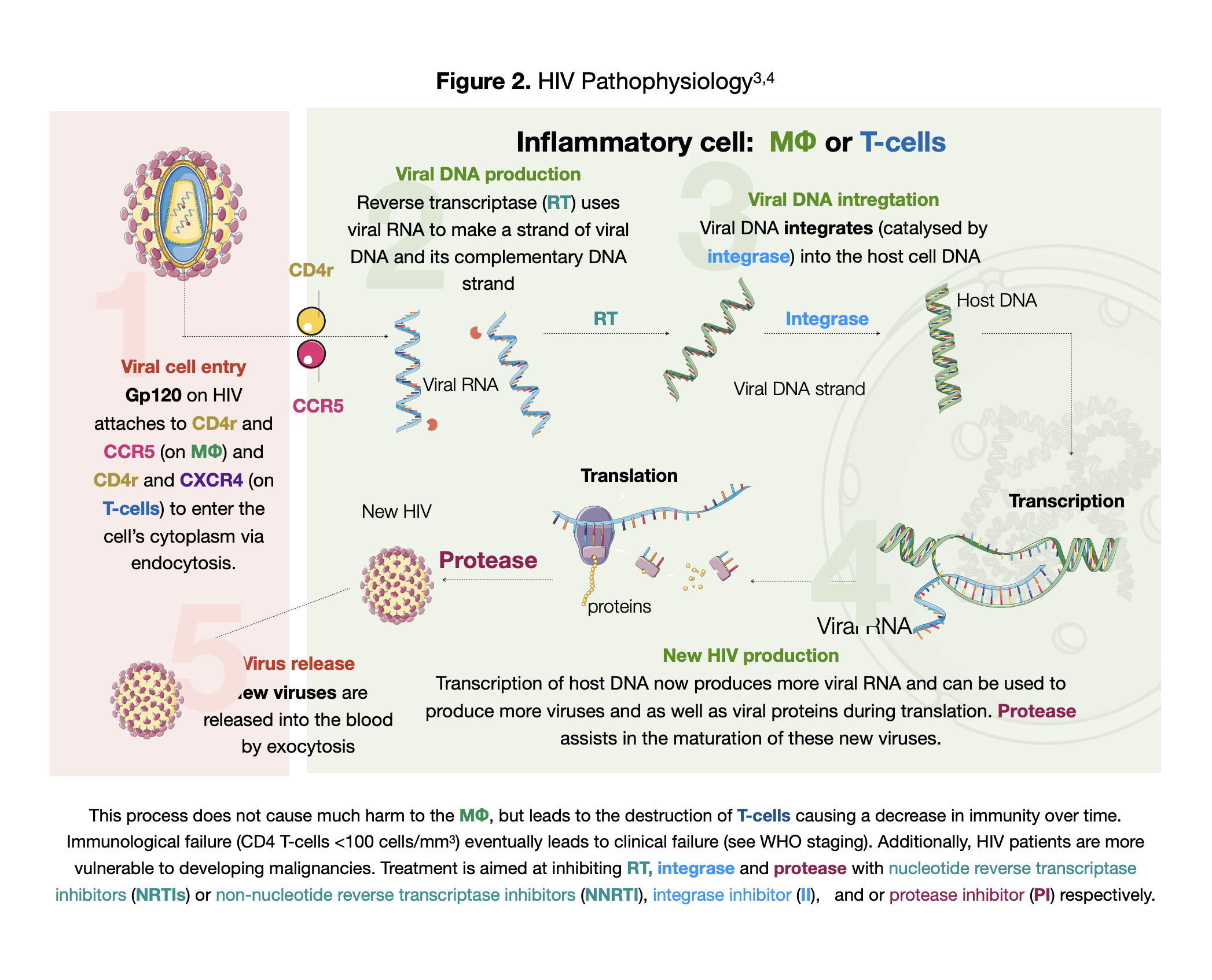
- Viral cell entry: Gp120 on HIV attaches to CD4r and CCR5 (on MΦ) and CD4r and CXCR4 (on T-cells) to enter the cell’s cytoplasm via endocytosis.
- Viral DNA production: Reverse transcriptase (RT) uses viral RNA to make a strand of viral DNA and its complementary DNA strand
- Viral DNA integration: Viral DNA integrates (catalysed by integrase) into the host cell DNA
- New HIV production: Transcription of host DNA now produces more viral RNA and can be used to produce more viruses and as well as viral proteins during translation. Protease assists in the maturation of these new viruses.
- Virus release: New viruses are released into the blood by exocytosis
Management considerations
Non-pharmacological
- Counselling, disclosing to partner(s) and reducing risky behaviours if any
Pharmacological Baseline investigations to assess treatment eligibility
- If GXP+, defer ART 2 – 8 weeks after initiating TB treatment (see local guidelines as it depends on TB drug sensitivity, whether TB is neurological vs non-neurological, and based on CD4 count)
- If CrAg+, but CSF negative for CCM, initiate ART 2 weeks after starting empiric anti-fungal treatment
- If HepBsAg+, include TDF in treatment regimen
- Ensure ALT is normal before initiating treatment. If not, correct the cause.
- Ensure a normal eGFR before starting TDF, or consider an alternative NRTI.
Anti-retroviral therapy (ART) = 2 NRTIs + INSTI or NNRTI or PI
- Adolescents & adults: 1st line TDF + 3TC + DTG (TLD) → 2nd line TDF + 3TC + LPV/r
- Children: 1st line ABC + 3TC + DTG (ALD) → 2nd line ABC + 3TC + LPV/r
- Renal friendly regimen: ABC + 3TC (low dose) + DTG
Second-line ART: Consider changing to a 2nd line regimen if VL >1000 copies/mL. Before changing regimens, make sure that there has been treatment adherence. Non-adherence itself can be a cause of a high VL.
Opportunistic infections
- INH prophylaxis is recommended for ALL HIV positive individuals, regardless of CD4 count/ Clinical stage
- Cotrimoxazole preventative therapy (CPT) is recommended in all children over 5, and adults with CD4 counts <200 or WHO Stage 2, 3, or 4 disease
References
- Dr G Bhanu Prakash Animated Medical Videos. How the HIV Infection Cycle Works – Animated microbiology. YouTube. January 31, 2019. Accessed on July 11, 2024. www.youtube.com/watch?v=GyofqO1TRjU
- Gilroy S & Faragon JJ. HIV infection and AIDS. July 8, 2021. Accessed September 9, 2021. https://emedicine.medscape.com/article/211316-overview
- HIV and AIDS in South Africa. April 15, 2020. Accessed September 9, 2021. https://www.avert.org/professionals/hiv-around-world/sub-saharan-africa/south-africa
- HIV risk behaviours. December, 2015. Accessed September 9, 202. https://www.cdc.gov/hiv/risk/estimates/riskbehaviors.html
- Images modified from using Servier Medical Art (https://smart.servier.com/) licensed under a Creative Commons Attribution 3.0 unported license (https://creativecommons.org/licenses/by/3.0/)
- South African ART Clinical Guidelines 2023