CARDIAC DOMINANCE
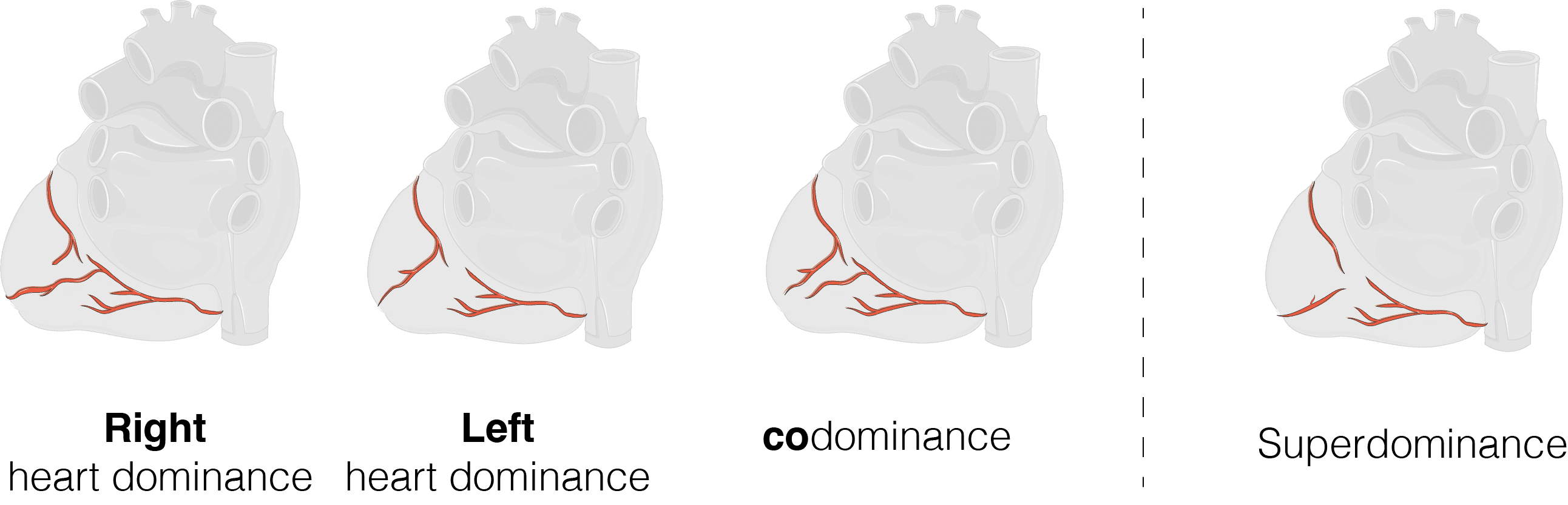
Cardiac dominance refers to which coronary artery supplies the posterior descending artery (PDA). The PDA supplies the inferior and posterior wall of the heart, the posterior portion of the interventricular septum and it typically supplies the AV node. There are largely 3 variations of cardiac dominance (A-C). These include:
- Right heart dominance (most common with a prevalence of 80-85%): Origin of the PDA is from the right coronary artery (RCA)
- Left heart dominance: Origin of the PDA is from the left circumflex artery (LCx)
- Codominance: The PDA is supplied by both the right coronary artery (RCA) and the left circumflex artery (LCx)
- “Super-dominance” is a rare 4th variant where the left anterior descending artery supplies the PDA.
CLINICAL APPLICATION
Occlusion of the PDA may cause the following: inferior +- posterior infarction and decreased perfusion to the AV node which may present with an AV block (also known as a heart block).
REFERENCES
- Shahoud JS, Ambalavanan M, Tivakaran VS. Cardiac Dominance. [Updated 2022 Sep 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK537207/
- Images modified using Servier Medical Art (https://smart.servier.com/) licensed under a Creative Commons Attribution 3.0 unported license (https://creativecommons.org/licenses/by/3.0/)